



August - September 2002 : Auditory Neuropathy/Dys-Synchrony. I. Diagnosis


- Details
- Category: Guest editorial
- Last Updated on Wednesday, 02 April 2014 13:25
- Written by Thierry MOrlet PhD
- Hits: 5175
1. Introduction
This month’s editorial is dedicated to a recently described new type of hearing impairment, Auditory Neuropathy/Dys-Synchrony (AN/AD). It is not until recently that this specific kind of deafness was identified by experienced audiologists and scientists using new techniques of exploration of the auditory system such as otoacoustic emissions (OAEs).
We will address first the definition of AN/AD and the necessary diagnostic tools and, in a future editorial, we will address the question of its management.
2. What is Auditory Neuropathy / Dys-Synchrony?
AN/AD is a type of hearing impairment that is characterized by:
- absence of auditory brainstem responses (ABRs) associated with the presence of a cochlear microphonic.
- presence of evoked OAEs (transient OAEs or distortion product OAEs)
- a pure tone audiogram that varies from normal to profound.
- disturbed speech perception inconsistent with audiogram and particular difficulty with speech in competing signals.
- absence of middle ear reflexes
- no efferent suppression of OAEs.
It is noteworthy to notice that a patient with AN/AD can have an audiogram of 90dBHL but still have OAEs and, alternately, a patient with AN/AD can have an audiogram in which all thresholds fall within the normal range of hearing, yet have no ABRs.
While cases with the symptoms of AN/AD were reported in the literature in the early 1980s (Worthington & Peters, 1980, Lenhardt, 1981, Kraus et al., 1984), the use of the term auditory neuropathy did not become prevalent until over a decade later (Starr et al., 1996). With hindsight we realize that we saw our first AN/AD patient at Kresge Hearing Research Laboratory in 1982. A boy of 14 years presented with no synchronous ABR, nearly normal though fluctuating pure tone thresholds, and relatively normal speech and language development. There were no neurological or motor deficits, and the patient’s complaints mimicked those of a patient with a central auditory processing disorder. His primary complaint was difficulty hearing in background noise or the presence of any competing signal. OAEs were not available in 1982 to further define his hearing ability, and he remained largely a mystery until several years later when additional patients with similar symptoms were identified.
Figure 1 shows the TEOAEs recorded in the right ear of a 10-year-old child and Figure 2 the ABR recordings. For the ABR, the two upper traces (in red) clearly show absence of any identifiable neural components, but the inversion of the polarity of the click stimulus reveal the presence of a long ringing cochlear microphonic that could have been improperly associated with a neural response if only one polarity of the click had been used.
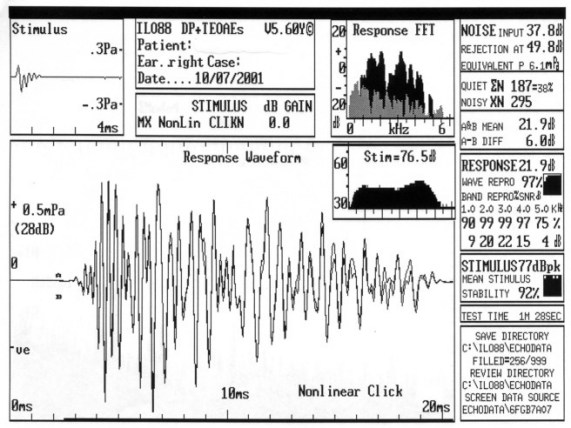
Figure 1: TEOAE response

Figure 2: ABR recording
Patients with results that were seemingly just as incongruous were identified by several facilities in the United States and Canada. These patients were reminiscent of those with inexplicably absent ABRs and normal pure tones (Worthington & Peters, 1980, Kraus et al., 1984).
Once AN/AD was defined as a hearing disorder, some basic criteria for making the diagnosis could be established. Sininger and Oba (2001) suggest that patients must have all of the following to be considered as having AN/AD: (1) evidence of poor auditory function, with difficulty hearing in at least some situations or for some stimuli, (2) evidence of poor auditory neural function, with absent or elevated auditory brain-stem reflexes (either middle ear muscle reflex or olivocochlear reflex) and an abnormal ABR, and (3) evidence of normal hair cell function, demonstrated by the presence of OAEs and/or cochlear microphonic (CM).
3. What is the CM?
An electrical response from the cochlea, the cochlear microphonic (CM) reflects a combination of inner and outer hair cell function. The CM can be identified by comparing auditory evoked potential averages obtained with both rarefaction and condensation clicks. Because the CM is a stimulus following response, it will reverse in phase with changes in the stimulus polarity from rarefaction to condensation (Ferraro & Krishnan, 1997). The appearance is that the waves "flip" or invert. For click and high frequency tone bursts, neural responses do not invert with stimulus polarity changes while the CM does. This comparison can also be used to distinguish wave I of the ABR from the CM because wave I may shift slightly in latency but does not invert. The CM in AN/AD patients has been noted to often be large and extend over a considerable time period. In some cases it may extend for several milliseconds and have the "appearance" of an ABR response (Berlin et al., 1998; Deltenre et al., 1999). This enhanced CM seems to be more pronounced with younger patients. Starr et al. (2001) found that the amplitude of the CM in AN/AD cases was greater in patients aged 10 years or younger when compared to normal hearing subjects. When a patient is suspected of having AN/AD, we recommend that a set of tests be administered first for proper classification of the hearing loss: middle ear muscle reflexes (MEMRs), OAEs, and ABRs with two polarities (Berlin, 1999). Notice that the presence of AN/AD does not rule out the possibility of cochlear loss or of a conductive component, and there can be several confounding factors that may make the diagnosis more difficult.
4. Can OAEs be absent in some cases of AN/AD?
Yes. Absence of OAEs can be found when a conductive problem exists. If OAEs are attempted but not obtained in this case, then the status of outer cell function remains unknown. Obtaining accurate results in ABR or ECochG in these cases is important in identifying the presence of hair cell responses. In patients with conductive components, sound must travel through a compromised middle ear system to reach the cochlea, and any resultant OAEs must return through the same system. Cochlear microphonics are measured via electrodes on the scalp and thus spared the return trip through a compromised middle-ear system, making it possible to obtain CM in some patients where OAEs are absent (Hood et al., 2002). For surface recorded responses, insert earphones can help reduce stimulus artifact and aid in identification of the CM. Also, another factor that can confound the diagnosis of AN/AD is hearing aid use. OAEs may be absent or greatly reduced in patients who have worn hearing aids over a period of time. Since some AN/AD patients naturally lose their emissions over time, use of hearing aids in both ears makes it more difficult to tell whether absence of OAEs is occurring naturally or as a result of hearing aid use and excess amplification. We have followed a number of patients who had robust OAEs at birth or when they were first identified as AN/AD but later lost their emissions. Such patients who otherwise meet the criteria of having AN/AD but have no OAEs have been reported by others as well (Deltenre et al., 1999; Rance et al., 1999). Recently, a study of transient otoacoustic emissions (TEOAEs), CMs, and summating potentials in 33 AN/AD subjects found that eight had absent TEOAEs bilaterally and three had absent TEOAEs unilaterally (Starr et al., 2001). From this group, nine had present TEOAEs on prior tests and all were prior hearing aid users. CMs were present in all the ears with absent TEOAEs.
5. What is the exact cause of AN/AD?
In AN/AD patients the exact site of the problem is not yet specified. Based on audiologic test results, the anatomic site of lesion of AN/AD lies somewhere in the auditory pathway between the outer hair cells and the afferent neurons of the auditory nerve. Locating the exact site of lesion is complicated by the likelihood that AN/AD has more than one etiology and by the tendency for secondary degenerative effects to occur as a result of damage to one part of the peripheral auditory system (Harrison, 2001). Proposed causes of AN/AD have been: (1) a disorder of the auditory nerve with normal outer hair cell function (such as peripheral hereditary motor-sensory neuropathy, Charcot-Marie-Tooth disease) (2) a disorder of the inner hair cells, or (3) a disorder of the synapse between inner hair cells and the eighth nerve dendrites (Berlin et al., 1993; Harrison, 1998; Starr et al., 1996, 2001). As more data are collected, it may be possible to define different types of AN/AD with varying prognostic and managerial implications.
Thorough birth and family histories can also provide insight into the diagnosis of AN/AD. Many patients identified with AN/AD have complicated birth histories, often having spent some time in the neonatal intensive care unit. In our first sample of 100 patients, we saw the following in birth histories of AN/AD patients: elevated bilirubin levels, prematurity, ototoxic medications, exchange transfusions, and oxygen deprivation requiring use of a vent. Mitochondrial disorders and neurological conditions such as cerebral palsy were also noted (Berlin et al., 2001).
The number of AN/AD patients with elevated bilirubin levels is not disproportionate to the number of babies with elevated bilirubin who do not develop hearing loss. More notable is the number of infants with AN/AD who have had exchange transfusions (Hood et al., 2002). From the sample of 100 patients reviewed by Berlin et al. (2001), 30 patients had jaundice while 25 had other complicating medical conditions such as cerebral palsy. However, many in this sample had no other complicating condition aside from AN/AD. This is interesting when compared to the group presented in the Starr et al. (1996) paper in which most patients did have some form of peripheral neuropathy. While AN/AD may occur in conjunction with a peripheral neuropathy, it is important to note that it can occur without any co-existing medical factors.
6. Can all newborn hearing screenings detect AN/AD?
The answer is no. Because AN/AD subjects have OAEs (and newborns do not wear hearing aids), any newborn hearing screening using ONLY OAEs (TEOAEs or DPOAEs) as an assessment tool will not be able to identify AN/AD. Notice also that when ABRs are used without inversion of click polarities, a long and large CM might be misread as an ABR response and an AN/AD case missed. OAE use in screening has the advantage of being a fast and low-cost technique to operate in a nursery. If OAEs can not be used in conjunction with ABRs for all well-babies, we recommend however that at least babies with at least one risk factor for hearing (as described by international committees) been checked using both techniques. If this procedure is followed, then it must still be realized that some AN/AD cases –those with no risk factors- will be missed.
7. References
- Berlin, C.I., Hood, L.J., Cecola, P., Jackson, D.F., & Szabo, P. (1993). Does type I afferent neuron dysfunction reveal itself through lack of efferent suppression? Hear. Res. 65, 40-50.
- Berlin, C.I., Hood, L.J., Hurley, A., & Wen, H. (1996). Hearing aids: Only for hearing impaired patients with abnormal otoacoustic emissions. In C.I. Berlin (Ed.), Hair cells and hearing aids. San Diego: Singular Publishing Group, Inc., 99-111.
- Berlin, C.I., Bordelon, J., St. John, P., Wilensky, D., Hurley, A., Kluka, E., & Hood, L.J. (1998). Reversing click polarity may uncover auditory neuropathy in infants. Ear Hear. 19, 37-47.
- Berlin, C. (1999). Auditory neuropathy: Using OAEs and ABRs from screening to management. Seminars in Hearing, 20(4), 307-315.
- Berlin, C.I., Taylor-Jeanfreau, J., Hood, L.J., Morlet, T., Keats, BJ (2001). Managing and renaming auditory neuropathy (AN) as part of a continuum of auditory dys-synchrony (AD). Abstracts ARO, 486, 137.
- Berlin, C., Hood, L., & Rose, K. (2001). On renaming auditory neuropathy as auditory dys-synchrony. Audiology Today, 13, 15-17.
- Deltenre, P., Mansbach, A.L., Bozet, C., Christiaens, F., Barthelemy, Pl, Paulissen, D., & Renglet, T., (1999). Auditory neuropathy with preserved cochlear microphonics and secondary loss of otoacoustic emissions. Audiol. 38, 187-195.
- Ferraro, J.A., & Krishnan, G. (1997). Cochlear Potentials in clinical audiology. Audiol. Neuro-Otol. 2, 214-256.
- Harrison, R.V. (1998). An animal model of auditory neuropathy. Ear Hear. 19, 355-361.
- Harrison, R. (2001). Models of auditory neuropathy based on inner hair cell damage. In Y. Sininger & A. Starr (Eds.), Auditory Neuropathy: A new perspective on Hearing Disorders (pp. 51-66). San Diego, CA: Singular Publishing Group, Inc.
- Hood, L.J., Berlin, C.I., Morlet, T., Brashears, S., Rose, K., & Tedesco, S. (In press, 2002). Considerations in the Clinical Evaluation of Auditory Neuropathy/Auditory Dys-synchrony. Seminars in Hearing.
- Kraus, N. Ozdamar, O., Stein, L., & Reed, N. (1984). Absent auditory brain stem response: Peripheral hearing loss or brain stem dysfunction? Laryngoscope, 94, 400-406.
- Lenhardt, M. (1981). Childhood central auditory processing disorder with brainstem evoked response verification. Arch. Otolaryngol. 107, 623-625.
- Rance, G., Beer, D.E., Cone-Wesson, B., Shepherd, R.K., Dowell, R.C., King, A.M. Rickards, F.W., & Clark, G.M. (1999). Clinical findings for a group of infants and young children with auditory neuropathy. Ear Hear. 20, 238-252.
- Sininger, Y., & Oba, S. (2001). Patients with auditory neuropathy: Who are they and what can they hear? In Y. Sininger & A. Starr (Eds.), Auditory Neuropathy: A new perspective on Hearing Disorders (pp. 15-35). San Diego, CA: Singular Publishing Group, Inc.
- Starr, A., Picton, T.W., Siniger, Y., Hood, L.J., & Berlin, C.I. (1996). Auditory neuropathy. Brain. 119, 741-753.
- Starr, A., Sininger, Y., Nguyen, T., Michalewski, H.J., Oba, S., & Abdala, C. (2001). Cochlear receptor (microphonic and summating potentials, otoacoustic emissions) and auditory pathway (auditory brain stem potentials) activity in auditory neuropathy. Ear Hear. 22, 91-99.
- Worthington, D., & Peters, J. (1980). Quantifiable hearing and no ABR: Paradox or error? Ear Hear. 5, 281-285.
8. For more information
Linda J. Hood Ph.D or This email address is being protected from spambots. You need JavaScript enabled to view it. :
Kresge Hearing Research Laboratory of the South
Department of Otolaryngology and Biocommunication
Louisiana State University Health Science Center
533 Bolivar Street New Orleans, LA 70112-2234, USA