Prediction
of cochlear pure-tone threshold and cochlear compression by means of extrapolated
DPOAE I/O-functions
Thomas Janssen, Ph.D.
ENT-Department, Technical University Munich, Germany
Due to their non-linear transmission characteristics and corresponding intermodulation distortion, outer hair cells evoke intermodulation vibrations in cochlear micromechanics and fluid when stimulated by two tones f1 and f2 (f2 > f1) of neighboring frequencies. In humans, the 2f1-f2 distortion product (DPOAE) has the highest amplitude and is therefore primarily used for diagnosing cochlear dysfunction. There are two main problems when using DPOAEs as a probe for monitoring loss of sensitivity and loss of compression of the outer hair cell amplifiers.

Fig. 1. Schematic drawing of how to evoke DPOAEs within
the cochlea and how to measure them in the outer ear canal. The sound probe
consists of two loudspeakers for applying the primary tones with frequencies
f1 and f2 and levels L1 and L2, and one microphone for measuring
acoustic signals in the outer canal. DPOAEs are generated within the region
of overlap of the traveling waves of the two primary tones close to the f2 place. The level
Ldp of the 2f1-f2 DPOAE and the related noise
floor (average of 6 spectral lines around 2f1-f2) are measures for
determining DPOAE amplitude and signal-to-noise ratio.
1. First problem: How to elicit DPOAEs?
DPOAE amplitude is known to depend on the frequency ratio and level ratio of the two primary tones. If we want to use DPOAEs as a probe for monitoring changes in outer hair cell function we need to ensure that DPOAE generation is restricted to a distinct place in the cochlea. The question is: what is the best parameter setting for eliciting DPOAEs? Intermodulation distortion originates in the cochlear region where the travelling waves of the two primary tones overlap. Due to the steeper slope of the travelling wave towards cochlear apex, the maximum interaction site is close to the f2 place in the cochlea. Thus, the outer hair cells of the f2 place contribute most to DPOAE generation (Fig. 1). The number of outer hair cells contributing to DPOAE generation depends on the size of the overlapping region which is determined by the levels L1 and L2 and the frequency ratio f2/f1 of the primary tones. To preserve the overlapping region at low primary tone levels for eliciting DPOAEs near the hearing threshold, a primary tone level setting has to be used that accounts for the different compression of the two primary tones at the DPOAE generation site, at f2. When using such a paradigm, the level and frequency of the higher primary tone (L2 and f2) are decisive for the generation of DPOAEs in the cochlea. Thus, when plotting the DPOAE level Ldp as a function of L2 (DPOAE I/O-function) DPOAEs reflect the compressive sound processing of the cochlea at the f2-place.
2. Using the scissor paradigm for eliciting DPOAEs.
How
must a parameter setting look like that accounts for the different compression
of the two primary tones? Whitehead
et al. (1995a) and our group (Janssen
et al., 1995a,b; Kummer et al., 2000) have proposed a primary
tone level setting in which the difference between L1 and L2
increases with decreasing stimulus level. Using this paradigm, instead of the
common used equilevel paradigm, DPOAE growth reflects the compressive nonlinear
cochlear sound processing known from direct measurements of basilar membrane
motion in animal experiments (Ruggero et al.,
1997; Boege and Janssen, 2002). Fig. 2 shows
the influence of the primary tone level difference on DPOAE level. As one can
see not the L1=L2 condition yields the highest DP level,
but the scissor pradigm. At high primary tone levels, L1 and L2
are equal. However, with lower stimulus levels the difference between L1
and L2 has to be increased using the formular L1=0.4L2+39
(with f2/f1=1.2). This so called scissor paradigm (in
German: “Pegelschere”, Janssen et al., 1995 a,b)
varies only slightly with f2 (Kummer
et al., 2000). Thus, the formular L1=0.4L2+39
can be used nearly independent of f2. It should be emphazised, that
this formular is only true for the sound probe (ER-10C, Etymotic Research, USA)
and the sound pressure calibration method (in-the-ear calibration, see Whitehead
et al., 1995b) used during the development of the scissor paradigm.
Thus, when using different sound probes and/or different calibration methods
a new scissor paradigm has to be determined. This is also true when measuring
DPOAEs in different mammalian ears (for guinea-pigs, see Michaelis
et al., to be published in Hearing Res).
L1 L2
65 65
63 60
61 55
59 50
57 45
55 40
53 35
51 30
49 25
47 20
Fig. 2. Scissor paradigm (left). DPOAE level Ldp for different
L1, L2 combinations. DPOAEs when elicited by the scissor
paradigm yielded highest levels (see projection on the floor). Dashed line on
the floor indicates equilevel primary tone setting (after Janssen
et al., 1995 a,b; Kummer et al., 2000).
3.
Second problem: How to measure DPOAEs at near-to-threshold primary tone levels?
At near-to-threshold primary tone levels either no DPOAEs or DPOAEs with unsufficient signal-to-noise ratios can be measured. Therefore, when plotting the DPOAE level Ldp as a function of f2 (DP-gram) the DPOAEs often do not reflect cochlear hearing thresholds. How to overcome the problem? The idea is as follows. If we can not reliably measure DPOAEs at close-to-threshold primary tone levels, then we have to estimate the DPOAEs at threshold. A simple way to estimate DPOAEs at threshold is to extrapolate DPOAE I/O-functions. For extrapolating DPOAE I/O-functions we need to know the relationship between the DPOAE level Ldp and the primary tone level L2
4.
Using extrapolated DPOAE I/O-functions for estimating DPOAEs at threshold.
Using the scissor paradigm L1=0.4L2+39dB in most of the DPOAE I/O-functions recorded in normal-hearing human ears a logarithmic dependency of the distortion product sound pressure level LDP on the sound pressure level L2 of the f2 primary tone can be found (Boege and Janssen, 2002). In normal-hearing ears, in the low primary tone level range the slope amounted to about 1 dB/dB whereas in the high primary tone level range the slope amounted to about 1/3 dB/dB. With increasing hearing loss the slope continously increases (see Janssen et al., 1998; Kummer et al., 1998 for mean slope values in normal-hearing and cochlear impaired subjects). With that, DPOAE growth is similar to that what has been found in basilar membrane responses (Ruggero et al., 1997). Thus, DPOAE I/O-functions are able to reflect the compressive sound amplification in the cochlea at the outer hair cell level.

Fig.
3. DPOAE I/O-function in a semi-logarithmic scale at f2 = 1709 Hz in a human cochlear hearing loss ear
(upper panel) and log-log scale (lower panel). Solid line shows the fitted linear
function. The vertical bar marks the estimated DPOAE threshold. Filled circles
indicate DPOAEs, open triangles noise floor (after
Boege and Janssen, 2002).
The logarithmic dependency of the DPOAE sound pressure level on the primary tone sound pressure level results in a linear dependency between the DPOAE sound presure pDP and the primary tone sound pressure level L2. In Fig. 3 the DPOAE sound pressure pDP (top panel) and the DPOAE sound pressure level LDP (bottom panel) of the same DPOAE I/O-function are plotted as a function of the primary tone level L2. The linear fit to the data (solid line) proves the logarithmic dependency of pDP on p2 or Ldp on L2. The correlation coefficient r2 gives a measure of the accuracy of the linear fit. The vertical bar marks the intersection point of the regression line with the primary tone level axis which serves as an estimate of the cochlear pure-tone threshold in both panels. (The estimated cochlear pure-tone threshold LEDPT is the extrapolated value equivalent to the primary tone level L2 that would give a zero DPOAE sound pressure (pDP =0).)
5.
Correlation between estimated DPOAE threshold and behavioral threshold.
In our clinical data set we found a close correspondence between the estimated cochlear pure-tone threshold and the behavioral threshold which was recorded with the same sound probe.
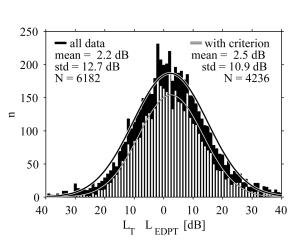
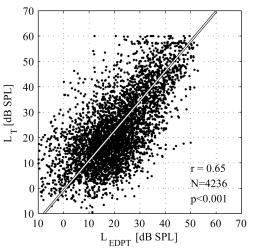
Fig. 4. Behavioral
pure-tone threshold LT is plotted across estimated DPOAE threshold
level LEDPT for 4236 DPOAE I/O-functions of 30 normal-hearing and
119 cochlear hearing loss ears fullfillung linear regression criteria (left).
Distribution of the difference between between pure-tone threshold LT
and estimated DPOAE threshold level LEDPT (right) (after Boege and Janssen,
2002).
When comparing the behavioral pure-tone threshold LT and the estimated cochlear pure-tone threshold LEDPT for 4236 DPOAE I/O-functions of 30 normal-hearing and 119 cochlear hearing loss ears that fulfill linear regression criteria (for detail see Boege and Janssen, 2002) a significant correlation is present. Moreover, there is almost a 1:1 relationship between the subjective and the objective measures. This means that there is a direct quantitative relationship between the estimated cochlear pure-tone threshold and the behavioral pure-tone threshold (Fig. 4, left). When calculating the difference for all 6182 as well as for the 4236 I/O-functions fulfilling the criteria the mean difference amounted to 2.2 and 2.5 dB, respectively. The standard deviations were 12.7 and 10.9 dB, respectively (Fig. 4, right).
Recently, Gorga et al. (2003) extended our method by increasing the primary tone level (up to 85 dB SPL) and changing the criteria for accepting I/O-functions. They also evaluated the effects of the primary tone frequency. The authors essentially replicated our results (Boege and Janssen, 2002) when using the same stimulus conditions and linear regression criteria. Taking measurements for a wider range of levels and slightly altering the inclusion criteria Gorga et al. achieved an improvement in test performance. They found prediction errors not to be uniformly distributed across test frequency. Best performance was observed for mid-to-high frequencies. In a retrospective study on our data using weighted extrapolated DPOAE I/O-functions we got similar results and attributed the frequency dependent estimation error to problems with in-the-ear-canal sound pressure calibration (Oswald and Janssen, 2003). Therefore, further efforts are necessary to improve the sound pressure calibration in the outer ear canal for applying definite sound pressure at the ear drum and hence improving cochlear pure-tone threshold estimation.
6.
Using the slope of the DPOAE I/O-functions
for estimating cochlear compression.
Besides
the estimation of pure-tone thresholds, DPOAE I/O-functions provide an additional
measure. That is the slope of the I/O-function, which is able to estimate the
compression of outer hair cell amplifiers. This was shown for guinea pigs in
which the outer hair cells were impaired using acute furosemide intoxication
(Mills and Rubel, 1996) and for
humans suffering from cochlear hearing loss (Janssen
et al., 1998; Kummer et al., 1998; Boege and Janssen, 2002; Neely et al., 2003).
In these studies the slope of the DPOAE I/O-function increases with increasing
hearing loss revealing loss of compression of outer hair cell amplifiers.
7.
Potential clinical applications of extrapolated DPOAE I/O-functions
An
important problem in neonatal hearing screening is to interprete the effect
of middle-ear status on the measures. Recently, we applied extrapolated DPOAE
I/O-functions in human neonates to estimate cochlear pure-tone threshold and
compression (Janssen et al., 2003).
The estimated pure-tone threshold was found to be increased within the early
postnatal period (average age: 3 days), predominantly at the higher frequencies,
and to be normalised in a follow-up measurement (after four weeks). However,
the slope of DPOAE I/O-functions obtained in the first and second measurement
was unchanged revealing normal cochlear compression. Consequently, we interprete
the findings as temporary sound conductive hearing loss due to amniotic fluid
and/or Eustachian tube dysfunction. Thus, we conclude that newborn hearing screening,
especially during the first days of life, may lead to false positive results
due to a temporary sound conductive hearing loss. In order to avoid unnecessary
and time consuming audiological testings we propose to use the slope of DPOAE
I/O-functions in neonatal hearing screening to differentiate between (temporary)
middle ear and (persisting) cochlear disorders.
We believe that extrapolated DPOAE
I/O-functions give more information for diagnostical purposes than those of
DP-grams or transitory evoked OEAs (TEOAEs). Beside the assessment of middle-ear
status we suggest our method to be able to quantify loss of cochlear sensitivity
and compression especially in newborns and children. Consequently, our future
targets are to implement extrapolated DPOAE I/O-functions in a hand-held hearing
screening device to provide frequency-specific and quantitative information
on hearing loss and to estimate whether there is a sound conductive or cochlear hearing
loss. Another potential application of extrapolated DPOAE I/O-functions is to
objectively adjust hearing aids in children. Since DPOAE I/O-functions are reported
to be correlated with loudness (Neely et al. 2003),
DPOAE would also offer the potentiality of basic hearing aid adjustment (Müller
and Janssen, in preparation).
Literature:
Boege P, Janssen
T (2002) Pure-tone threshold estimation from extrapolated distortion product
otoacoustic emission I/O-functions in normal and cochlear hearing loss ears.
J Acoust Soc Am 111 (4) 1810-1818
Gorga MP, Neely ST, Dorn PA, Hoover BM (2003) Further efforts to predict
pure-tone thresholds from distortion product otoacoustic emission input/output
functions. J Acoust Soc Am 113 (6) 3275-3284
Janssen
T, Kummer P, Arnold W (1995a) Wachstumsverhalten der Distorsionsproduktemissionen
bei kochleären Hörstörungen. Otorhinolaryngol NOVA 5:34-46
Janssen
T, Kummer P, Arnold W (1995b) Wachstumsverhalten der Distorsionsproduktemissionen
bei normaler Hörfunktion. Otorhinolaryngol NOVA 5:211-222
Janssen T, Kummer P, Arnold W (1998) Growth behavior
of the 2f1-f2 distortion product otoacoustic emission in tinnitus. J
Acoust Soc Am Vol 103 (6):3418-3430
Janssen
T, Klein A, Gehr D. (2003) Automatische Hörschwellenbestimung bei Neugeborenen
mit extrapolierten DPOAE-Wachstumsfunktionen. Eine neue Hörscreening-Methode.
HNO (to be published in December)
Kummer P, Janssen T, Arnold W (1998) The level
and growth behavior of the 2f1-f2 distortion product otoacoustic emission and
its relationship to auditory sensitivity in normal hearing and cochlear hearing
loss.
J Acoust Soc Am Vol 103 (6):3431-3444
Kummer P, Janssen T, Hulin P, Arnold W (2000) Optimal
L1-L2 primary tone level separation remains independent of test frequency in
humans. Hearing Research 146: 47-56
Michaelis CE, Gehr
DD, Deingruber K, Arnold W, Lamm K. Optimum primary tone
level setting for measuring high amplitude DPOAEs in guinea pigs (to be published
in Hearing Res)
Mills DM, Rubel ED (1996). Developement of the cochlear amplifier. J Acoust Soc Am Vol 100: 428-441
Müller J,
Janssen T. Similarity in loudness and distortion product otoacoustic emission
input/output functions: Implications for an objective hearing aid adjustment
(in preparation)
Neely ST, Gorga MP,
Dorn PA (2003) Cochlear compresion estimates from measurements of distortion-product
otoacoustic emissions. J Acoust Soc Am Vol 114: 1499-1507
Oswald JA, Janssen T (2003) Weighted DPOAE I/O-functions: A tool
for automatically assessing hearing loss in clinical application. Z Med Physik 13: 93-98
Ruggero MA, Rich NC, Recio A, Narayan SS (1997) Basilarmembrane responses
to tones at the base of the chinchilla cochlea. J Acoust Soc Am Vol 101: 2151-2163
Whitehead ML, McCoy MJ, Lonsbury-Martin BL, Martin GK (1995a) Dependence
of distortion-product otoacoustic emissions in primary tone level in normal
and impaired ears. I. Effects of decreasing
L2 below L1. J Acoust Soc Am 97: 2346-2358
Whitehead ML, Stagner BB, Lonsbury-Martin BL, Martin GK (1995b) Effects
of era-canal standing waves on measurements of distortion-product otoacoustic
emissions. J Acoust Soc Am 98: 3202-3214
 |
•
•
•
• Main
|
 |